
Mapping the path of the Pandemic

The current misplaced concerns about the impending fourth wave of Covid-19 in India, is a fallout of lack of robust thought leaders with firsthand battle experience in transmission dynamics of communicable diseases. To predict whether we will have a disastrous fourth wave, let us go back to fundamentals of transmission dynamics of communicable diseases which any epidemiologist who has worked at the ground level will know……….
By Dr Amitav Banerjee
What about India? Will we have a fourth wave?
India has willy-nilly gone through widespread community transmission rendering vast swathes of its population robustly immune. Studies have established that naturally acquired immunity is 13 to 26 times stronger than vaccine induced immunity. This can be long lasting due to T and memory cells after waning of antibody levels. Studies from Singapore and Sweden have shown that individuals had cellular immunity against SARS-CoV-2, 17 years after encountering SARS-CoV-1.
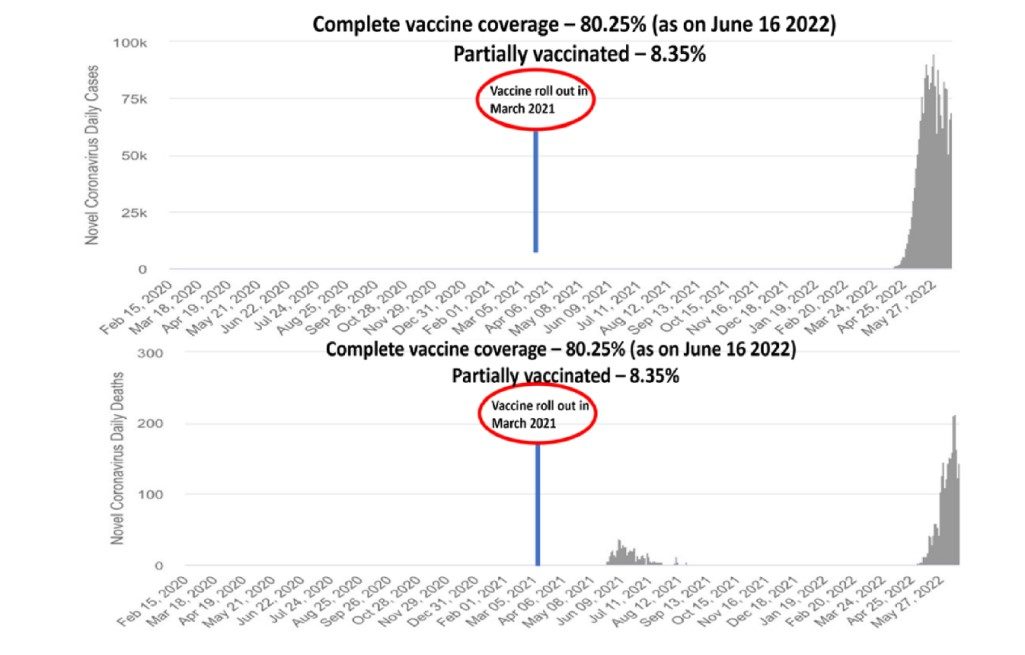
What explains the episodic spike in cases in major metropolitan cities like, Delhi, Mumbai, etc? Does it signal an imminent fourth wave? Metropolises and big cities the world over are business, tourist and educational hubs. The high level of population movement due to this disturbs the immunological equilibrium from time to time resulting in surges which are of no consequence.
The phenomenon can be compared to a deck of cards. Shuffling or adding new cards could disturb the arrangement. In the past, people lived in relatively closed communities with less number of people entering or going out. These communities were like an un-shuffled deck of cards. Closed communities also attain herd immunities faster.

On the positive side, most migrants are young and healthy so most infections will be asymptomatic or mild and hardly of any consequence. At this stage of the pandemic we should stop focusing on number of cases and positivity rates and monitor hospital admissions and deaths in the young and healthy rather than the elderly or people with co-morbidities most of whom die “with the virus” rather than “due to the virus.”
It can be understand that tropical diseases, particularly the communicable diseases, should have been the forte of Indian doctors. Post independence they should have come into their own dictating strategies for communicable disease control at the global level. Alas this was not to be, as the profession continued to imitate their erstwhile masters, the present lot of whom having little firsthand experience in tropical medicine and infectious diseases.
The history of the rise and fall of tropical medicine is closely linked with the fortunes of the British Empire. The health of its sailors and soldiers played a major role in establish British Imperialism throughout the world. James Lind, a British Naval Surgeon in 1747, discovered that consumption of lime prevented scurvy, the bane of sailors. Adding lemon and oranges to the rations of British sailors, which earned them the nickname of “limey,” changed the course of world history. British sailors sailed far and wide laying the foundations of the British Empire.
On land, the British in the process of expanding their colonial dominion in India and many developing countries laid great emphasis on tropical medicine and communicable diseases during the 17th and 18th centuries. Tropical medicine, including study of communicable diseases, evolved as a by-product of the British Raj. The discipline was fallout of the exploitation by the colonial rulers who wanted to safeguard the health of the British personnel occupying distant lands.
During the 19th century, when the British Empire was fast expanding, Joseph Chamberlain, Secretary of State for these colonies, emphasised training of British doctors in communicable diseases occurring among the “servants of the Raj.” Chamberlain visualised that without conquering disease “constructive Imperialism” will not be possible. He believed that tropical medicine was vital for British economic and social dominance – to the extent of it being a colonial science.
Sir Ronald Ross’s research on transmission of malaria in 1897, work for which was done in India, and which earned the India born researcher a Noble and a knighthood, further gave a fillip to research in tropical medicine in India. Chamberlain remarked, “The man who shall successfully grapple with this foe of humanity and find the cure for malaria, for the fever desolating our colonies and shall make the colonies liveable for white men will do more for the world, more for the British Empire, than the man who adds a new province to the wide Dominion of the Queen.”
With the downfall of the British Empire after the Second World War, the importance given to infectious diseases declined. Better standards of living in the West eliminated these diseases in their native country. And since the rulers did not occupy foreign lands, research in tropical medicine and infectious diseases lost its pride of place which was at its peak during the British Raj.
The colonial rulers played a game of chess, in which the control of communicable diseases was important to conserve their chessmen on the board. Once the game was over with the fall of the British Raj, they lost interest.
However, Sir Patrick Manson, author of the classic, “Manson’s Tropical Diseases,” said, “The tropical practitioner enjoys opportunities for original research and discovery far superior in novelty and interest to those at the command of his fellow inquirer in the well worked field of European and American research.”
Had Indian researchers followed this legacy, we would have been at the forefront in planning strategies in the fight against the present Covid-19 pandemic. On the contrary, Indian researchers and policy makers followed the West in this pandemic. The blind led the blind. Pandemic operations on war footing calls for experienced leadership of high calibre on par with that required for military campaigns. Military campaigns have potential for immense harm if not executed smartly. Same with pandemic strategies have gone awry.
Kurt von Hammerskin-Equord, a German general and a staunch opponent of Hitler and the Nazis, gave a classification of military leadership styles. “I distinguish four types. They are clever, hardworking, stupid, and lazy officers. Usually two characteristics are combined. Some are clever and hardworking: their place is the general staff in planning. The next ones are stupid and lazy; they make up 90 percent of every army and are suited to routine duties. Anyone who is both clever and lazy is qualified for the highest leadership duties, because he possesses the mental clarity and strength of nerve necessary for difficult decisions. One must beware of anyone who is both stupid and hardworking; he must not be entrusted with any responsibility because he will always cause damage.”

Unfortunately, in this pandemic, we have had hardworking but clueless medical leadership from the West. Their efforts, as well as those of their imitators, caused immense collateral harm besides fracturing society due to closure of businesses, educational institutions and isolating people.
The current misplaced concerns about the impending fourth wave of Covid-19 in India, is a fallout of this lack of robust thought leaders with firsthand battle experience in transmission dynamics of communicable diseases.
To predict whether we will have a disastrous fourth wave, let us go back to fundamentals of transmission dynamics of communicable diseases which any epidemiologist who has worked at the ground level will know. Of course these nuances will elude the “mouse-click epidemiologists” generating fancy mathematical models with incomplete inputs.
When an infection enters a virgin population, it has the potential to spread like a forest fire if not stamped out in the beginning. Resource intensive measures such as contact tracing, testing of asymptomatic and isolation are important to prevent the establishment of community transmission. These measures were destined to fail for a highly contagious respiratory virus. In fact, countries which did well in the beginning to check infections and spread of community transmission are currently having very high levels of infections and deaths in spite of of mass vaccination, for e.g. Taiwan.
(The author is a former epidemiologist who led the Mobile Epidemic Team of the Indian Armed Forces and currently, Professor and Head, Community Medicine, Dr DY Patil Medical College, Pune)