
Covid-19 Current Concerns
 The current scenario of Covid-19 in all over the world is like fix eyes on the ball and this bouncer will pass by harmlessly…
The current scenario of Covid-19 in all over the world is like fix eyes on the ball and this bouncer will pass by harmlessly…
By Dr Amitav Banerjee
In response to reports of Covid-19 surge in many countries, particularly China & Japan, the Ministry of Health and Family Welfare, Government of India, issued fresh guidelines reiterating the fivefold strategy of test-track-treat-vaccinate and Covid Appropriate Behaviour, which supposedly controlled the covid-19 situation in the country in the past. An added advisory recommends genomic surveillance for emerging variants of concern. The government also decided to re-introduce random testing of International passengers at airports.
It is always prudent to err on the side of safety. Having said this, we should not remove our eyes from the ball and also constantly monitor the pitch.
First let us keep our eyes on the ball and judge its pace. In relation to the pandemic the ball is the novel corona virus and its pace is the lethality. The lethality of the corona virus was grossly overestimated by the pace by which it killed the tail-enders i.e. the elderly and the vulnerable, in the nursing homes of Europe early in the pandemic. One paper in Lancet put the ball mark at 20%. Such estimates appearing in high impact journals and mathematical models from Imperial College, London predicting doomsday caused panic which was sustained in spite of subsequent studies which established the infection fatality rates to be many times lower.
A number of serosurveys few months into the pandemic estimated the global Infection Fatality Rate (IFR) with the original Wuhan virus, to be around 0.3% and lower still in countries of Africa and Asia.
The pace of the ball has slowed considerably due to loss of shine and loss of grass on the pitch!
As the pandemic progressed, the pace of the ball, i.e. the IFR has gone down steeply, due to many factors like mutation to less virulent strains (Omicron), and increasing population level immunity particularly after natural infections which confers 13 times more robust immunity compared to vaccine.
A recent meta-analysis by investigators from Stanford University have found infection fatality rates to be in the range of 0.0003% till the age of 19 years, and even in the old say a 69 year old, the infection fatality rate ranged from 0.03% to 0.07% . The royal heirs have turned into commoners – the novel corona virus is as mild as the other circulating corona viruses which causes common cold and is novel no more. Do we need to panic?
 Do we run after the ball after it has crossed the boundary line?
Do we run after the ball after it has crossed the boundary line?
Our country is an ocean of people living and working in very crowded conditions. Almost all have recovered from natural infection. Even in the earlier phase of the pandemic the “test, trace, isolate” did not save many runs. Only a miniscule fraction of infections could be detected by this costly strategy. We have data to support this statement. In June 2021, serosurvey by the Indian Council of Medical Research (ICMR), revealed that 67.7% of Indian had antibodies, a marker of past infections. From this we can estimate that a staggering 92 crores people had had covid-19 whether they experienced symptoms or not. At this point of time according to official records only 3 crores cases were detected by the “test, track, isolate, treat” strategy.
The vaccination cover of our population was 5% in June. From this we can infer that by the intensive testing and tracing efforts we detected 4% of cases while we missing 96%. Is it worth the effort to go for this strategy at the fag end of the pandemic when the virus has become so much milder? But for the fear of the term “corona” like that associated with “Gabbar Singh” in “Sholay” for all practical purposes we are chasing a common cold – Gabbar Singh has lost his hands and has aged as well! Fear him no more. Similarly, we should debate whether genomic surveillance would yield any information which would guide policy. The “new variant” suspected to be circulating in China and supposedly a threat to other countries has been identified in over 90 countries, including India where it was detected in July 2022! Testing passengers at airports and other such measures would be like closing the stable door after the horse has bolted.

Jo dar gaya, samjho woh mar gaya! (The one who panics, consider him dead!)
This filmy dialogue from “Sholay” may appear trite and trivial. On a serious note, a paper published by Centre for Disease Control (CDC), Atlanta, showed that among 540, 667 adults hospitalized with Covid-19, anxiety and fear-related disorders were the highest risk factors after obesity leading to severe disease and death. We cannot forget the Indian experience during the second wave when panic fueled by irresponsible media resulted in a medical stampede contributing to many deaths by overwhelming our health services.
A vicious cycle of panic-unavailability of beds-panic may have been responsible for many deaths during the second wave if we follow this paper from CDC. Against this background, we should check the 24 x 7 media hype which can again generate similar panic and adversely affect the health of our people. While it is understandable that the Centre has issued the present guidelines as a precautionary measure, the media should not read too much into it and convert molehills into mountains.
 Do we keep giving repeated overs to a bowler who is not taking any wickets?
Do we keep giving repeated overs to a bowler who is not taking any wickets?
A fast bowler may make an impact when the ball is new and the pitch has grass. As the ball loses shine and the pitch breaks the same bowler will be less effective. On the contrary he may give away valuable runs. Similarly data from all over the world is indicating that Covid-19 vaccines lose impact at population level very rapidly. The figure below gives the data of trends of cases and deaths in Japan [Fig 1, Fig 2], one of the countries facing surge in Covid-19 cases (as usual, there is no data from China which would suggest a crisis there!).
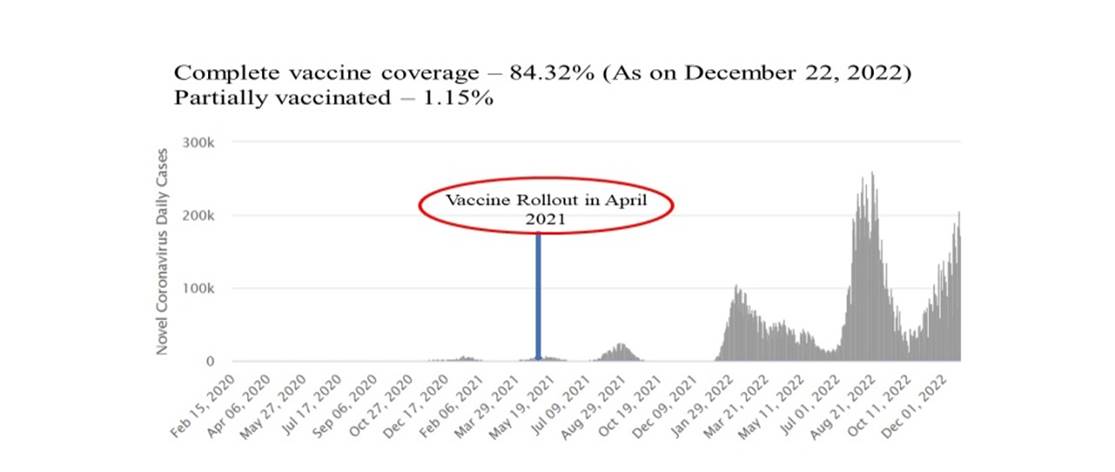
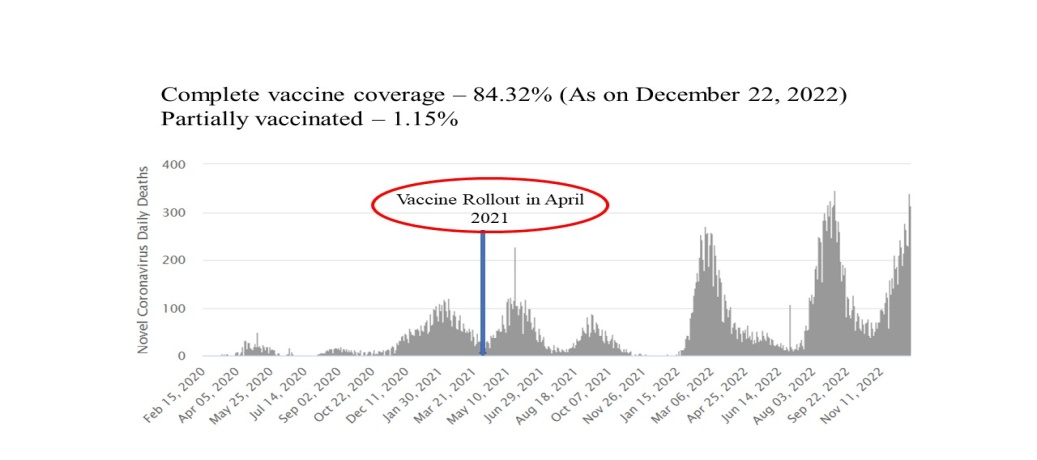
It is obvious from the above figures that both the cases and the deaths due to covid-19 have spiked in Japan after the mass vaccination roll out. Even with over 80% vaccination coverage and boosters Japan is facing a surge. Similar phenomena have been seen from Singapore, South Korea, Taiwan, Malaysia, Sri Lanka and other countries with very high vaccination cover. In fact some virologists have also expressed concerns that selection pressure due to mass vaccination during a pandemic can trigger evolution of mutant strains.
It is well known that new variants like Omicron and its sub variants evade vaccine induced immunity. So why persist with mass vaccination and advisory for boosters which are made from older variants.

The grass on the pitch – countries like China which had very harsh restrictive measures still have lot of grass on the pitch which will let the ball rip through, i.e. virgin population who have not been exposed to the natural virus. The present surge therefore is to be expected and it will come down as fast as it goes up. Countries like India where majority of the population has acquired immunity after recovery from natural infection have no cause for worry. Not only will the grassless pitch not encounter a wave there will not even be a ripple.
Do we try to dismiss a batsman who is not making in runs?
As mentioned a recent meta-analysis has estimated the lethality of the virus at 0.0003% in young people and 0.03% to 0.07% in people who are 69 years old. We do not try to dismiss a batsman who is not scoring runs in limited over cricket. Can a resource constrained country like India afford to go all out to dismiss the corona virus which has lost all sheen after incarnation as Omicron.
 The strategy based on evidence – shield the tail-enders
The strategy based on evidence – shield the tail-enders
A good captain shields the tail-enders from fast as well as slow bowlers, spin can be tricky! Similarly strategy should be to shield the vulnerable with co-morbidities and the frail elderly by looking after their overall health and vaccination on recommendation of their personal physicians.
Conclusion
The centre should review their guidelines after a week or ten days and withdraw them if there is not even a ripple, which is most likely. The accumulated and current evidence does not support any of the recommendations in the guidelines and will be resource intensive and generate undue panic in the population due to media hype.
(The author is Clinical Epidemiologist and currently Professor and Head, Community Medicine at DY Patil Medical College, Pune.)