
Mitigating Hearing Impairment
Special – World Hearing Day 2017
Mitigating
Hearing Impairment
Society for Sound Hearing is making a significant contribution towards effective delivery of primary ear and hearing care by organising frequent awareness and screening camps

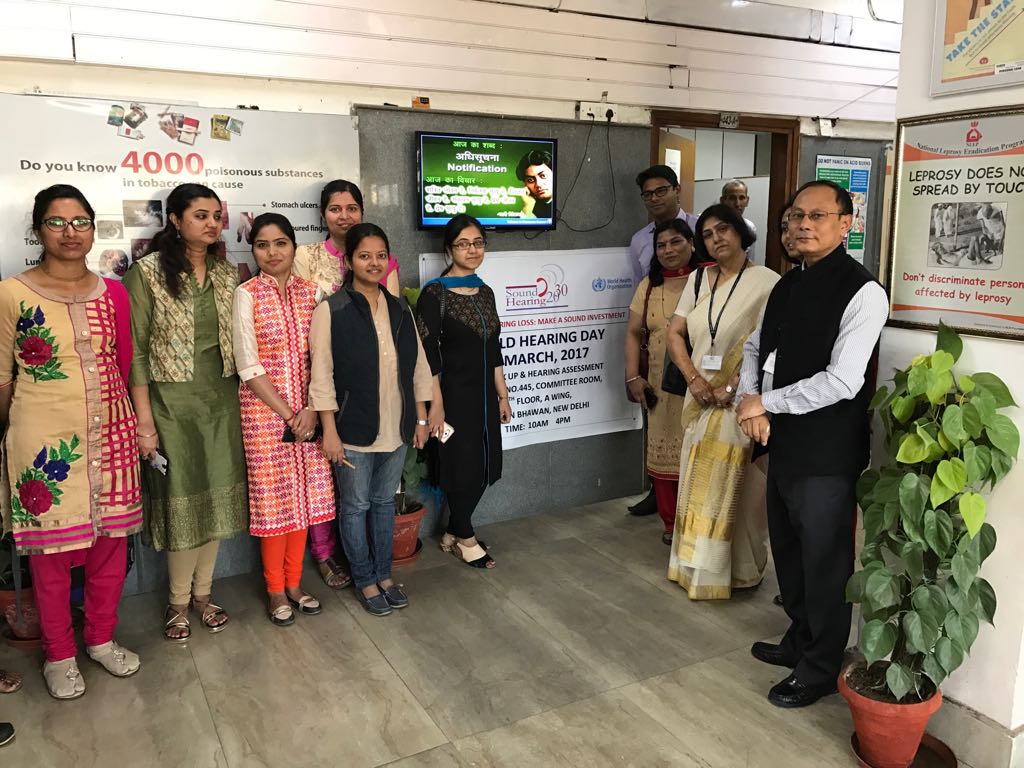
On the occasion of World Hearing Day 2017, an ear awareness & screening camp was organized by Society for Sound Hearing in collaboration with Department of Community Medicine and Department of ENT, Maulana Azad Medical College, Lady Harding Medical College, New Delhi and ALPS International and Ministry of Health & Family Welfare, Govt. of India at Nirman Bhawan, New Delhi.
It was inaugurated by CK Mishra, Secretary, Ministry of Health & Family Welfare, Govt. of India. While Dr. Promila Gupta, DDG, Ministry of Health and Family Welfare, Govt. Of India, facilitated the conduct of the screening programme along with Dr A.K. Agarwal, Professor of Excellence, former Dean, MAMC, New Delhi, President, Sound Hearing 2030 and Dr Suneela Garg, Director-Professor & Head, Community Medicine, MAMC, New Delhi and Hony Secretary General, Sound Hearing 2030.
As part of screening program, 286 beneficiaries were screened. 57% of the people screened were females while 43% were males. The age of the patients varied from 25 years to 60 years. The participants were first screened for hearing problem using case history sheet. This was followed by ear examination by ENT specialists and those requiring audiometric assessment were further evaluated in a separate room by audiometrists from ALPS International. Out of the total people screened, 21.53% of the people were found to have some form of ear morbidities.
 Out of the total of 286 individuals screened, records of 195 individuals were analysed since the remaining did not submit the records. The results of 195 individuals showed that diminished hearing was seen in 19 individuals (10%), wax impaction in 14 individuals (7%) Chronic Suppurative Otitis Media in 9 individuals (5%) and normal in 153 individuals (78%). All the beneficiaries screened were counselled by doctors from Maulana Azad Medical College, Delhi. The patients who were found to be suffering from ear problems were referred for further treatment to government hospitals in Delhi.
Out of the total of 286 individuals screened, records of 195 individuals were analysed since the remaining did not submit the records. The results of 195 individuals showed that diminished hearing was seen in 19 individuals (10%), wax impaction in 14 individuals (7%) Chronic Suppurative Otitis Media in 9 individuals (5%) and normal in 153 individuals (78%). All the beneficiaries screened were counselled by doctors from Maulana Azad Medical College, Delhi. The patients who were found to be suffering from ear problems were referred for further treatment to government hospitals in Delhi.
Ear infections occur most commonly in young children because they have short and narrow Eustachian tubes. Infants who are bottle-fed also have a higher incidence of ear infections than their breastfed counterparts. Other factors that increase the risk of developing an ear infection are altitude, changes, climate changes, exposure to cigarette smoke, pacifier use and recent illness or ear infection.
Ear infections occur when one of patient’s Eustachian tubes becomes swollen or blocked and fluid builds up in its middle ear. Eustachian tubes are small tubes that run from each ear directly to the back of the throat. The causes of Eustachian tube blockage include allergies, colds, sinus infections, excess mucus, tobacco smoking and infected or swollen adenoids (tissue near tonsils that trap harmful bacteria and viruses).
 Mild pain or discomfort inside the ear, a feeling of pressure inside the ear that persists, fussiness in young infants, pus-like ear drainage and hearing loss are common symptoms of ear infections. These symptoms might persist or come and go. Symptoms may occur in one or both ears. Chronic ear infection symptoms may be less noticeable than those of acute ear infections.
Mild pain or discomfort inside the ear, a feeling of pressure inside the ear that persists, fussiness in young infants, pus-like ear drainage and hearing loss are common symptoms of ear infections. These symptoms might persist or come and go. Symptoms may occur in one or both ears. Chronic ear infection symptoms may be less noticeable than those of acute ear infections.
Children younger than six months who have a fever or ear infection symptoms should see a doctor. Always seek medical attention if your child has a fever higher than 102 degrees or severe ear pain. Childhood onset hearing loss can be congenital or as a sequel to infections such as otitis media, meningitis, rubella etc. Adult onset hearing loss can be a result of age (presbycusis) and noise induced hearing loss. WHO classification classifies hearing impairment according to pure tone averages in the better hearing ear. The following table shows the WHO grades in hearing impairment. There are over 360 million persons in the world living with disabling hearing loss. Out of these 32 million are children. Many more suffer with lesser degrees of hearing loss. Most of those with hearing loss live in developing countries. Amongst the countries of the WHO South-East Asia region, the prevalence of disabling hearing loss varies from 4.2% to 16.6%.The reported prevalence in India is 6%. Based on this, it is estimated that over 70 million persons in India are living with hearing loss equal to or greater than moderate degree.
 In recently held awareness camps, experts including Dr. M. Meghachandra Singh, Director-Professor, Department of Community Medicine, Dr Vipra Mangla and others examined ears of govt employees. Most of them complained redness, air bubbles, or pus-like fluid inside the middle ear, fluid draining from the middle ear, a perforation and a bulging or collapse in the eardrum
In recently held awareness camps, experts including Dr. M. Meghachandra Singh, Director-Professor, Department of Community Medicine, Dr Vipra Mangla and others examined ears of govt employees. Most of them complained redness, air bubbles, or pus-like fluid inside the middle ear, fluid draining from the middle ear, a perforation and a bulging or collapse in the eardrum
According to Dr A.K. Agarwal, Professor of Excellence, Former Dean, MAMC, New Delhi, and President, Sound Hearing 2030, hearing loss is one of the most common sensory impairments affecting the population worldwide. In developing countries, children with hearing loss or deafness rarely receive schooling. Persons living with disabilities, including hearing loss, also have a much higher unemployment rate. Exclusion from communication can lead to feelings of isolation, loneliness and depression. Besides these, hearing loss affects social and economic development in communities and countries.
Morbidities which are associated with hearing loss, such as impacted wax and chronic otitis media are frequently encountered in the community. Chronic suppurative otitis media (CSOM) is one of the most common infectious diseases of childhood. It is characterized by presence of persistent discharge from the ear. The prevalence of this condition varies from 1% to 46% across the world.
As per WHO, 65–330 million individuals across the world are suffering with ‘draining ears.’ More than half of those of those affected with CSOM develop significant hearing loss. Not only does this cause long-term effects on the development of language, auditory and cognitive skills, but it is also associated with many dangerous and life-threatening complications. This morbidity accounts for 28,000 deaths (in one year) and a disease burden of over 2 million DALYs. Over 90% of the burden is borne by countries of South-east Asia and Western Pacific regions, Africa, and ethnic minorities in the Pacific Rim.
Another clinical entity commonly encountered in the community is impacted wax. Wax is a normal secretion of the ear, but its impaction in the ear canal can lead to unpleasant symptoms and is occasionally associated with serious squeal, including hearing loss, social withdrawal, poor work function and perforated eardrums. This is a major cause of primary care consultations and treating impacted wax can pose a significant financial burden on governments.
As per WHO, 50% of all cases of hearing loss can be prevented. Based on the population strategy for prevention of diseases, it is essential that causative morbidities with high or moderate frequency of occurrence in the community and effective means of prevention and control should be targeted. In terms of hearing loss, this refers to common conditions such as chronic otitis media, ante-natal and peri-natal problems, wax, excessive noise, ototoxicity, meningitis, measles and mumps.
Prevention can take place at the primordial level through changes in behaviour and improved healthcare and at primary level through strategies for improved immunization, improved birth practices, prompt treatment of acute ear infections, avoidance of noise and judicious use of ototoxic medicines among others. Where ear morbidities have already developed and hearing loss has set in, effective secondary prevention can be undertaken through early detection. Early identification is important to ensure that persons with ear diseases and hearing loss can receive suitable management.
 Persons with ear morbidities, such as suppurative otitis media, otitis media with effusion and wax impaction can be benefitted through a variety of medical and/or surgical interventions. Those who do not benefit from such management techniques can be effectively rehabilitated, if suitable actions are initiated early. Use of hearing devices, such as hearing aids and cochlear implants can help many. Others may benefit from sign language education and other modalities.
Persons with ear morbidities, such as suppurative otitis media, otitis media with effusion and wax impaction can be benefitted through a variety of medical and/or surgical interventions. Those who do not benefit from such management techniques can be effectively rehabilitated, if suitable actions are initiated early. Use of hearing devices, such as hearing aids and cochlear implants can help many. Others may benefit from sign language education and other modalities.
A possible barrier to timely diagnosis and care is the lack of awareness about ear and hearing conditions. Most parents experience difficulties in recognizing hearing loss in their children, Delay in diagnosis and management of congenital hearing loss leads to significant adverse impact on the linguistic and academic outcome.
A variety of unhealthy beliefs and practices regarding ear care and ear conditions are widely prevalent in community. Self-cleaning of ear, use of home remedies and stigma attached to ear problems contributes to the high prevalence of these morbidities. Added to this is the lack of information about the consequences of common ear morbidities and their treatment. The situation is further aggravated by a lack of suitable human resources for ear and hearing care and poor availability of the required services at grassroots level. The paucity of services for primary ear care along with a lack of training resources, adds to the growing burden of ear diseases and hearing loss.
 World Health Assembly passed a resolution in 1995 for prevention of deafness which focuses on developing primary ear and hearing care services within countries, integrated within its primary health care system. The resolution encouraged the WHO Member States to develop their own programmes for prevention of deafness, which target its common causes through a primary health care system approach. India took its first step in this direction with the implementation of the National Programme for Prevention and Control of Deafness.
World Health Assembly passed a resolution in 1995 for prevention of deafness which focuses on developing primary ear and hearing care services within countries, integrated within its primary health care system. The resolution encouraged the WHO Member States to develop their own programmes for prevention of deafness, which target its common causes through a primary health care system approach. India took its first step in this direction with the implementation of the National Programme for Prevention and Control of Deafness.
The programme is currently being run in over 220 districts of India. Delhi was one of the pilot states which initiated the programme in two of its districts in 2006. The programme includes training and capacity development of human resources and provides suitable care for ear diseases and hearing loss at the primary and secondary levels of health care. There is a need to step up efforts towards effective delivery of primary ear and hearing care along with advancements in the field with affordable high tech care