The Monitoring Lapse
The true scale of rabies’ impact in India is shrouded in conflicting mortality statistics. The gap between the NCDC data, which reported 54 deaths, and the WHO estimate of 20,000 deaths in a year, indicates the apathy of policymakers in ensuring a robust surveillance system for a disease with 100 per cent fatality.
By Dr Amitav Banerjee
 Rabies, known as hydrophobia (fear of water), is a fatal zoonotic disease of the central nervous system, caused by a virus belonging to the family Lyssavirus Type 1. The transmission of the virus is sustained among warm-blooded animals, mostly carnivorous such as dogs, cats, jackals, and wolves. Bat rabies is a concern in some regions of the world. Man gets infected by bites or licks from rabid animals. The disease has a long and variable incubation period, a short spell of illness due to encephalomyelitis terminating in death, despite intensive care. It has a fatality rate of 100 per cent. The patient is hyperactive, hypersensitive and conscious throughout, making the end most painful and tragic.
Rabies, known as hydrophobia (fear of water), is a fatal zoonotic disease of the central nervous system, caused by a virus belonging to the family Lyssavirus Type 1. The transmission of the virus is sustained among warm-blooded animals, mostly carnivorous such as dogs, cats, jackals, and wolves. Bat rabies is a concern in some regions of the world. Man gets infected by bites or licks from rabid animals. The disease has a long and variable incubation period, a short spell of illness due to encephalomyelitis terminating in death, despite intensive care. It has a fatality rate of 100 per cent. The patient is hyperactive, hypersensitive and conscious throughout, making the end most painful and tragic.
Epidemiology
The main reservoir of the deadly rabies virus is in wildlife. This makes eradication impossible. Natural geographical boundaries and strict control of the entry of infected animals have sustained rabies-free status in some island nations such as Australia, Taiwan, Cyprus, Iceland, Ireland, Japan, Malta, New Zealand and the UK, among some others.
In India, the Union Territory of Lakshadweep and the Andaman and Nicobar Islands are rabies-free.
While wildlife maintains the reservoir of the virus, the source of infection with the rabies virus is from dogs in 99 per cent of human infections. Children are more vulnerable to dog bites and rabies.
The incubation period, the time lapse between the dog bite and the onset of symptoms, shows wide variations. It is usually 1–3 months but may range from seven days to years. It is shorter in extensive bites on the face, head, neck and upper extremities and bites from wild animals.
Once the virus gains entry, it multiplies in muscle or connective tissue at the site of the bite before it attaches to nerve endings and travels via the peripheral nerves to the central nervous system.
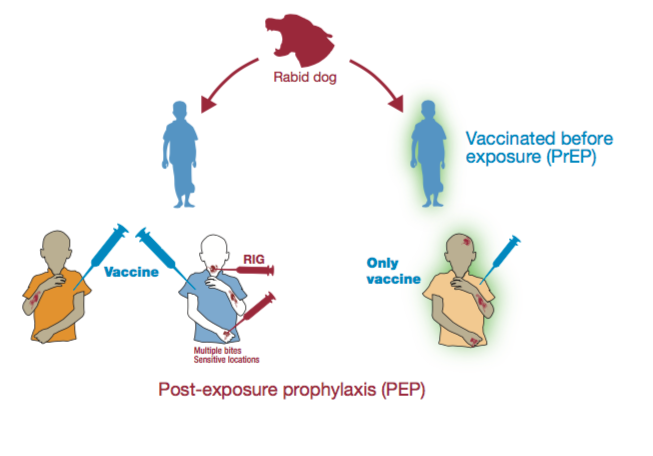
Post-exposure prophylaxis – wound care and first aid
First aid after an animal bite is most crucial in the prevention of rabies. It should be prompt and thorough since once the virus lodges to the peripheral nerve cells, the course to fatality is irreversible. It is a medical emergency and involves local wound treatment and the administration of rabies immunoglobulin and a course of vaccine when indicated.
The local treatment of the bite is of utmost importance to remove as much of the virus as possible from the site before it attaches to the nerve endings. Immediate flushing and washing of the wound and surrounding areas is urgently indicated using plenty of soap and running water. This should continue for at least 15 minutes. Unfortunately, this first aid is often delayed or denied. Following the wash, the application of alcohol or a 0.01 per cent solution of iodine or povidone iodine acts as a virucidal agent. Suturing of the wound should be avoided. Antibiotics and anti-tetanus toxoid should follow the local treatment.
Rabies immunoglobulin for passive immunisation is administered only once, preferably at, or as soon as possible after, the initiation of post-exposure vaccination. Beyond the seventh day after the first dose of rabies vaccine, immunoglobulin is not indicated because an active antibody response is expected to have occurred from the vaccine.
Rabies vaccines
The current generation of rabies vaccines are purified cell-culture vaccines (CCV) and embryonated egg-based vaccines (EEV). The dose and schedule depend on the category of exposure:
Category 1 exposure consists of touching, feeding of animals, or licks on intact skin. Vaccine is not indicated.
Category 2 exposure is licks over broken skin, minor scratches or abrasions without bleeding. These need immediate vaccination and local treatment of the wound.
Category 3 exposures are single or multiple bites or scratches, licks on broken skin, contamination of mucous membranes with saliva from licks, and contacts with bats. These types of exposure call for immediate vaccination and administration of rabies immunoglobulin after local wound treatment.

Contradictory Figures of rabies deaths in India
For a disease with 100 per cent fatality, one would have presumed that we would be having accurate figures about it at the national level. Surprisingly, the estimates of deaths from rabies in India vary drastically.
Official NCDC Data: The National Centre for Disease Control (NCDC) reported 54 suspected human rabies deaths in 2024, alongside over 3.7 million dog bite cases.
ICMR Study (2025): A recent ICMR study suggests a lower—but more realistic—estimate of over 5,700 annual deaths.
WHO Estimates: India has been cited as having up to 20,000 deaths annually, which is often quoted to highlight the massive burden.
Rising Death Trends: Despite some figures showing lower numbers, official parliamentary replies in 2025 noted a steep rise in recorded rabies deaths, increasing from 22 in 2022 to 180 in 2024, highlighting extreme variations in data reporting methods.
The wide range from NCDC data reporting 54 deaths in a year to the WHO estimate of 20,000 deaths is highly inconsistent and indicates the apathy of policymakers in ensuring a robust surveillance system for a disease with 100 per cent fatality. The estimates of 20,000 annual rabies deaths projected by the WHO need challenging by our government and call for transparency about the inputs on which this highly concerning estimate by the WHO is based.
If we cannot measure the burden accurately, how are we going to address it?
Robust surveillance and reliable data on rabies are urgently required for our country before we contemplate any future drastic strategy at huge investments such as the universal roll-out of pre-exposure prophylaxis by including rabies vaccine in the Universal Immunisation Program.
This is not a far-fetched contemplation as a recent paper in Lancet Regional Health South East Asia, by Lodha et al, titled, “Rabies Control in High Burden Countries: role of universal pre-exposure Immunisation” published in December 2023, presents the necessity and rationale for including pre-exposure immunisation with rabies vaccine in India’s national immunisation schedule. Obviously, this paper is going by the WHO’s estimate of 20,000 deaths from rabies in India every year.
Without any reliable data and the ridiculously high estimates by the WHO, launching such a public health program will amount to public health quackery.
In the interim, equitable access to post-exposure prophylaxis to augment energetic first aid of dog bites by training of all healthcare workers right up to the rural areas will prevent many deaths from rabies.
Proper availability and storage of rabies immunoglobulins and rabies vaccine right up to the Primary Health Centre level is also crucial.
Failures of Rabies Vaccines in India
While the rabies vaccine is effective when administered correctly, several factors in India have led to documented cases where individuals died despite being vaccinated. Recent reports from states like Kerala and Maharashtra highlight that most “vaccine failures” are actually due to deviations from standard medical protocols such as:
 Omission of Rabies Immunoglobulin (RIG): For Category III exposures (deep bites or bites with blood), the vaccine alone is insufficient because it takes 7–14 days to produce antibodies. RIG provides immediate passive immunity. Many deaths in India occurred when patients received the vaccine but were not given RIG.
Omission of Rabies Immunoglobulin (RIG): For Category III exposures (deep bites or bites with blood), the vaccine alone is insufficient because it takes 7–14 days to produce antibodies. RIG provides immediate passive immunity. Many deaths in India occurred when patients received the vaccine but were not given RIG.
Improper Wound Management: Failure to immediately wash the wound with soap and water for 15 minutes can lead to failure. This simple step can flush away a significant amount of the virus before it enters the nervous system.
Incorrect Injection Site: Medical guidelines strictly prohibit administering the vaccine in the gluteal muscle (buttocks) because the absorption rate is poor. Several deaths in India have been linked to this specific error by healthcare providers.
Anatomical Location of Bite: Bites on the face, head, or hands have a much shorter distance to the brain. In these cases, the virus may reach the central nervous system before the vaccine-induced antibodies can take effect.
Cold Chain Failure: Vaccines must be stored between 2°C and 8°C. Inconsistent electricity or poor management in smaller health facilities can render genuine vaccines ineffective.
Shortages and Quality Testing: Extreme shortages in some states have reportedly led to the distribution of vaccine batches before they could undergo full quality testing at the Central Drugs Laboratory.
Fake Rabies Vaccines: In recent years, more serious concerns regarding the vaccine supply chain and quality have emerged.
In late 2025, international health bodies including the CDC and Australian health authorities issued alerts about counterfeit batches of the popular Abhayrab vaccine circulating in major Indian cities.
The concerned manufacturer, Indian Immunologicals (IIL), did concede that in January 2025 it identified one batch in the market, Batch No. KA24014, with packaging that did not match the original. The company said it informed regulators in India and law enforcement agencies, lodged a complaint, and worked with authorities for action. IIL stated that this was one incident.
Fake drugs in the Indian markets are becoming a serious issue. Strengthening the drug control machinery with more inspectors and checks particularly for life-saving vaccines and drugs together with fast courts and stringent punishments for offenders is urgently required. Regrettably, our track record on regulatory control of quality of drugs is not commensurate with our aspiration of being the “pharmacy of the world”.
India’s Stray Dog Problem and high rates of dog bites
India reports over 3.7 million (37 lakh) dog bite cases annually. Recent government data indicated 37,17,336 reported dog bites in 2024, averaging over 10,000 cases per day. The majority of these bites are from stray dogs.
Control of stray dogs can also contribute in bringing down the cases of rabies in the country.
The Supreme Court (SC), on 11 August 2025, ordered all stray dogs to be removed from the streets of Delhi, the national capital, and housed in dedicated shelters under the arrangement of the concerned authorities, within eight weeks.

The SC ruling triggered heated debate and protest by animal activists. They declared the recommendations of the court impracticable as there are over 10 lakh stray dogs in Delhi with non-existent shelters. They further stated that confining them in crowded makeshift shelters can precipitate zoonoses, including the deadly rabies.
According to Maneka Gandhi, implementing the SC orders would need a colossal sum of Rs 15,000 crore. Besides, she said, the vacuum effect can draw other animals like rats and monkeys. Gandhi instead recommended strict enforcement and close monitoring of Animal Birth Control Centres (ABCs).
In response to these concerns, the SC made a U-turn following discussions on the issue, with the court emphasising the implementation of the existing Animal Birth Control Rules 2023. The SC withdrew its directives and called for a national strategy on the problem.
This flip-flop is the result of years of apathy. Lack of attention to the problem of stray dogs and other animals on our streets has resulted in this stalemate.
The ABC program, which appears to be the consensus of all stakeholders, would also require huge resources such as veterinary surgeons, operating rooms, dog catchers, supporting staff, and vehicles.
The Way Forward
We have few choices. We cannot wish away the problem. The ABC program should be implemented in letter and spirit, irrespective of the costs and resources involved. In addition, we have to have a reliable database on rabies cases and deaths, by initiating registries on digital platforms to generate real-time figures instead of gross estimates, which go widely off the mark and have the potential to drag us into drastic investments incurring huge costs such as universal pre-exposure immunisation against rabies.
We cannot put the cart before the horse. To launch such a program we should have robust surveillance and monitoring of rabies deaths and not depend on shortcuts like mathematical models which are increasingly being used by the current genre of laptop epidemiologists.