
The Silent Spike
 Once considered an adult-only ailment, hypertension is now quietly affecting children as young as newborns. It can lead to devastating consequences if left unchecked. Read on to know what you need to do to safeguard your child’s health.
Once considered an adult-only ailment, hypertension is now quietly affecting children as young as newborns. It can lead to devastating consequences if left unchecked. Read on to know what you need to do to safeguard your child’s health.
By Dr HP Singh /Dr Sachin Bhargav
A growing habit of sedentary lifestyle, lack of exercise, heavy consumption of fast food, , and intake of steroids either during pregnancy or from any other sources may lead to the problem of high blood pressure, commonly called hypertension, in children—and even in newborns. The problem may go undetected because, many times, there are no symptoms or signs of this disease. If left untreated, hypertension can lead to heart failure, vision problems, kidney failure, paralysis, and stroke early in life. It is a general belief that high blood pressure (hypertension) is a problem that affects only adults. Contrary to this belief, hypertension can be present at any age, even in newborns and young children. When parents learn that their child has hypertension, it is very natural for them to deny the possibility due to their ignorance. It is the responsibility of the paediatrician and the paediatric nephrologist to clear their doubts and to initiate an appropriate management plan.
Contrary to popular belief, high blood pressure does not spare the young. Approximately 2-5 per cent of children suffer from hypertension, and the majority are unaware they have it. The condition is especially prevalent among obese children, where rates soar to 10-30 per cent.
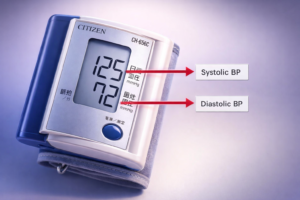
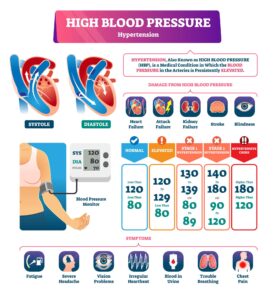
Blood pressure is the force of the blood against the walls of blood vessels as the heart pumps blood to various parts of the body. If this pressure becomes too high, the child is said to have high blood pressure or hypertension. As in adults, a child’s BP is read as two numbers. The first number, or systolic BP, is the pressure when the heart is pumping blood to various parts of the body. The second number, or diastolic BP, is the pressure when theheart is resting between beats. Diastolic BP is lower than systolic BP. A child is considered to be hypertensive when either the systolic, diastolic, or both blood pressures are high.
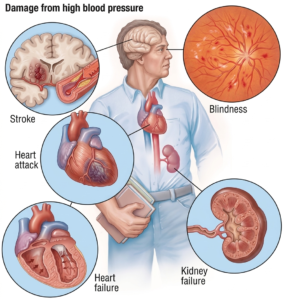
Often symptomless in its early stages, undetected hypertension can silently damage the heart, kidneys, eyes, and brain—leading to stroke or heart failure even in childhood. Regular check-ups, especially for children with risk factors like low birth weight, kidney disease, or a family history of hypertension, are essential for early detection.

The obese children are more prone to hypertension. If hypertension is allowed to continue or become worse over years, the prolonged extra pressure in the blood vessels can lead to heart failure, stroke, damage to eyes and kidney even in children.
A child’s blood pressure is not measured by adult standards. It varies with age, sex, and height, and is considered high only when it consistently exceeds the 95th percentile on standardised charts.
Normal BP is lower in children than in adults. BP increases with age and body size. Normal BP for a child will depend on the child’s age, sex and height. We compare your child’s BP to readings given on BP charts which lists normal BP or high BP for boys and girls based on their height and age. A child is said to be hypertensive if his average systolic or diastolic BP is more than 95th percentile (according to the standardized charts) for age, genderand height on more than 3 occasions. The doctor is the best person to read and interpret the charts. To label a child as hypertensive, BP charts have been issued by the fourth US task force report on hypertension .These are charts consulted by doctors to arrive at a conclusion whether the child has hypertension or not. Since these charts are difficult to interpret and not easily available to parents,it is recommended that if your child’s BP is beyond the values listed in the table here for the specific age group, you need to consult your doctor(paediatrician/paediatric nephrologist)
Child Blood Pressure (BP) – What is Normal?
Since these charts are difficult to interpret and not easily available to parents,it is recommended that if your child’s BP is beyond the values listed in the table here for the specific age group, you need to consult your doctor(paediatrician/paediatric nephrologist)Hypertension has been graded according to the B.P readingslike Prehypertension: – Blood pressure is > 90th percentile but <95th percentile (as per BP chart). Children in this range of BP should be carefully followed up as they grow up. And stage 1 hypertension (Unsafe):- BP exceeds 95th percentile up to 5 mm above 99th percentile. Blood pressure in this range should be rechecked at least twice in the next 1-3 week or even earlier. Stage 2 hypertension (Dangerous):- BP exceeds 5 mm or more above the 99th percentile. Confirmation should be made at the same visit.
Children who are more than 3 years and are seen at health care setting (for example cold, cough or fever) should have their blood pressure measured. Children who are less than 3 years should get their BP cheeked if they have:
- History of low birth weight, prematurity or requirement of neonatal intensive care,
- History of heart disease by birth
- History of recurrent urinary tract infection
- History of blood or protein loss in urine
- History of any kidney disease in the past
- Family history of kidney disease
- History of organ transplantation
- History of receiving medicines which can cause high blood pressure/kidney damage.
The usual symptoms of hypertension are headache (sometimes throbbing in nature), flushing, giddiness, bleeding from nose, vision disturbances, poor school performance, irritability, blood or protein in urine, passing urine more or less frequently and weight loss. In some cases hypertension can be without symptoms and therefore those children who are obese, have history of neonatal intensive care stay, or have kidney/ heart disease or cardiac disease should have their blood pressure checked.
For quick reference, parents should be concerned if BP readings cross 100/70 in children under five, 120/80 in those aged five to ten, and 130/90 in older children. If readings are high, they must be confirmed with the correct cuff size—too small or too large a cuff can give false results.
Generally it is preferred to check the blood pressure when the child is sitting comfortably in a chair with feet on the ground and the arm at the level of the heart. The BP cuff should be of the right size for the child’s age. The width of thecuff bladder (rubber inside the outer cloth) should be 40% of the arm circumference midway between the shoulder and elbow joint and the length should be double the width. Another simple way is to get a bladder cuff whose width covers ¾ of the upper arm. If the cuff size is not appropriate the blood pressure readings may come falsely high or low. However if an appropriate cuff size is not available the next bigger size can be used. Cuff sizes with a width of 4 cm, 9cm, 10cm, 13cm, and 20cm are available in the market. The usual symptoms of hypertension are headache (sometimes throbbing in nature), flushing, giddiness, bleeding from nose, vision disturbances, poor school performance, irritability, blood or protein in urine, passing urine more or less frequently and weight loss. In some cases hypertension can be without symptoms and therefore those children who are obese, have history of neonatal intensive care stay, or have kidney/ heart disease or cardiac disease should have their blood pressure checked. Mercury instruments are the best for checking blood pressure, but as they are being phased out, aneroid devices are being used more commonly and they are fairly accurate, but they require frequent calibration.Automatic BP machines are also being used.If an automatic (digital) blood pressure machine is being used and blood pressure readings come high, then they need to be confirmed with mercury or aneroid device.
AUTOMATIC BP MONITORING DEVICE
Ambulatory Blood Pressure Monitoring (ABPM)means blood pressureis recorded over a 24 hours period by a BP monitor where cuff is tied to the arm and a small digital blood pressure machine is attached to a belt around the waist. The child carries on his/her normal activities in the day and sleep with it, while the machine is on. The machine takes the blood pressure readings at regular intervals usually every 15-30 minutes during the day and night. The monitor should be kept on throughout the night. At the end of 24 hours the cuff and the machine are removed and given to the hospital for analysis of readings. For the machine to work properly, it is important to make sure that the tube attached to the machine is not twisted or bent. As a parent you are instructed to maintain a diary, to note the timing of going to bed, medication and general activities.There are a number of reasons why a doctor advises 24 hour ABPM , which are to find out if the high BP reading in the clinic is higher than the reading away from clinic e.g. home

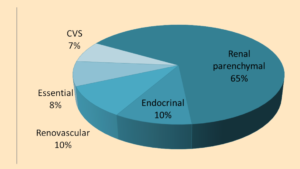
(called white coat hypertension), to see how well the medicines are working and whether they are controlling the blood pressure all the time and to see whether blood pressure at night is less than the recording during day time. In majority of young children an underlying cause of hypertension can be identified e.g. kidney, heart, blood vessels, hormone problems, tumour or drugs. Diseases of the kidney are the most common cause of hypertension in children. Primary or essential hypertension, commonly seen in adults, is becoming common in children, who are obese or over weight.
Causes of Hypertension
If a cause for hypertension is diagnosed, appropriate treatment can be initiated and the child may have normal blood pressure afterwards.
For few reasons, a child may have to remain on anti-hypertensive medicines throughout the life. Once a child is diagnosed to have hypertension, it is very important to evaluate any underlying disease and to find out risk factors for essential hypertension like obesity, smoking, alcohol, etc. In addition tests are required to find out if any complication (involvement of eye, heart or kidney) hasoccurred or not. The common tests which may be required arekidney function tests, hormone levels, lipid profile, urine examination, ultrasound and doppler test of kidney, kidney scan, echocardiogram, ECG and eye examination. Most children with essential hypertension require lifestyle modification swhich include weight reduction, meditation, yoga, exercise, low salt diet. Other risk factors like smoking, alcohol, steroids, oral contraceptives, sleep apnea should also be controlled. For secondary hypertension, surgery helps in certain cases,e.g. if any tumour is causing hypertension, then it needs to be removed surgically. Timely detection helps in appropriate treatment of hypertension and its cause and helps to prevent end organ damage in adult life.
Indications for drug treatment in hypertension
a) Stage 1 hypertension persisting even 6 months after lifestyle modifications or those who have any preexisting kidney disease
b) Stage 2 hypertension
c) Damage to eye, kidney, heart, or brain has occurred
d) Pre hypertension in a child with chronic kidney disease, diabetes or lipid abnormalities
LIFE STYLE MODIFICATION
Normal blood pressure values of Boys according to age and height | Normal blood pressure values of Girls according to age and height

Early diagnosis, lifestyle changes, and timely medical intervention can reverse or manage hypertension, preventing lifelong complications.
Childhood hypertension is no longer a rarity—it is a growing concern that demands parental awareness and proactive care. From maintaining a healthy weight and active lifestyle to regular blood pressure monitoring, small steps can make a big difference. Whether the cause is lifestyle-related or stems from an underlying condition like kidney disease, early detection is the key to protecting your child from a lifetime of health struggles. Consult your paediatrician, and take action before the silence becomes dangerous.