
Decoding the wrath of virus



An extensive study carried out by the authors to delineate the clinical characteristics and evaluate the prevalence of underlying factors of COVID-19 resulted in highly significant findings that merit close attention…
By Dr Prof Ramesh K. Goyal/ Dr Puneeta Ajmera/ Dr Jaseela Majeed
Today, India is virtually waging a war against coronavirus (COVID-19), the global pandemic that has ravaged the most parts of the world too. The United Nations has called corona pandemic the worst global humanitarian crisis since the World War II. The first case of coronavirus infection in India was detected on 30 January 2020 in Kerala. The patient, a student at the Wuhan University of China, was tested positive for novel coronavirus after returning to Kerala. The Government of India has taken the challenge head on by frontloading tough decisions from implementing “Janata Curfew” on 22 March 2020 to initiating nationwide lockdown from 25 March 2020 to May 17, 2020 urging 1.3 billion Indians to stay home to contain the spread of this deadly pandemic.
Accentuating factors of COVID-19
Literature review shows that there are very few studies that outline path physiology of c Also, its mechanism of transmission is still uncertain. Present knowledge relies on researches on similar corona viruses that describe human-to-human transmission through respiratory droplets. To compound the threat, association of corona with comorbidities like cardiovascular diseases, hypertension and diabetes increases the mortality rate from the infection.
The link of morbidities in COVID-19 with renin angiotensin system (RAS) and angiotensin converting enzyme-2 (ACE2) as the site of the multiplication of coronavirus has widely been reported. Delineating the clinical characteristics of corona infection with RAS cannot be undermined. There is a necessity to consider holistically the role of RAS when the ACE2 receptors are occupied by coronavirus. There is massive derangement of the entire RAS in corona infection and patients with pre-existing co-morbidities. ACE inhibitors or angiotensin receptor blockers should be monitored carefully considering the role of RAS in the prognosis of corona infections.
Exclusive DPSRU Study
Countries all over the world are taking aggressive steps and adopting all possible preventive measures to decrease the spread of COVID-19. Previous researches on SARS and MERS described the association of age, gender and presence of co-morbidities with mortality risk, with diabetes and cardiac diseases being the most imperative components to predict adverse outcomes. Therefore, it is necessary to evaluate these parameters in COVID-19 also.
We carried out a study to delineate the clinical characteristics and evaluate the prevalence of underlying comorbidities if any, in deceased corona victims in India. A literature search was conducted using different sources to collect the data pertaining to demographic, epidemiological, clinical and laboratory characteristics of deceased patients along with their medical history, travel and exposure history and underlying chronic diseases if any.
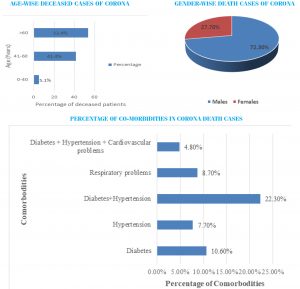
Using the database from the Union Ministry of Health and Family Welfare, and other official sources from 30 January (when the first COVID-19 case detected in India) to 10 April 2020, we conducted a retrospective multi-centre study on the first 206 death cases in India with laboratory-confirmed infection of SARS-CoV-2. Results depict that around 53.4 percent of deaths included people aged above 60 years which shows that older people are at significantly higher risk of developing corona infection. Males (72.3 percent) seemed to be hit harder and were more likely to have severe illness than females (27.7 percent). Pre-existing comorbidities like diabetes, hypertension, respiratory and cardiac problems were prevalent in around 54.1 percent of deceased and therefore strongly associated with poor outcome in corona affected patients in India. Patients having pre-existing comorbidities are more susceptible to develop several complications which highlights the significance of earlier cardiac monitoring and supportive care in such patients.
Background
In 2002, SARS-COVID was first spotted in the Guangdong province of China and recognized as the cause of severe acute respiratory syndrome outbreak with CFR (Case Fatality Rate) of 9.6 percent leading to 8096 confirmed SARS cases across 29 countries and 774 deaths. The symptoms of SARS-COVID included fever, cough, dyspnoea, and watery diarrhoea. Higher fatality rates were detected in elderly patients as well as patients with medical conditions like diabetes, hypertension, cardiac problems etc. Almost a decade after the SARS-COVID outbreak in September 2012, Middle East Respiratory Syndrome (MERS), caused by MERS corona virus (MERS-CoV) was detected in Saudi Arabia with CFR of 34.4 percent. MERS shared many symptoms with SARS like fever, atypical pneumonia, yet key differences are apparent. Noticeable gastrointestinal symptoms, acute respiratory distress syndrome (ARDS) and acute kidney failure were also reported in patients with MERS. Around 2494 confirmed MERS cases with 858 deaths were reported across 27 countries. All these cases were linked with residence or travelling to the regions near Arabian Peninsula with more than 80 percent involving Saudi Arabia ( the World Health Organization, 2004). In 2015 an outbreak of MERS was reported outside Arabian Peninsula in the Republic of Korea with confirmed cases in countries across Europe, North Africa, United States, Asia and the Middle East. By the end of 2016, more than 1850 laboratory-confirmed MERS-CoV cases were recorded, with a mortality rate of about 35 percent. Although CFRs of SARS and MERS are much higher, COVID-19 has resulted in more deaths because of large number of cases.
Fatal Association
The common symptoms of COVID-19 are fever, dry cough, nasal congestion, fatigue, diarrhoea, shortness of breath and breathing difficulty. In some cases disease may lead to more serious respiratory conditions like bronchitis, pneumonia, respiratory failure or multiple organ failure. The Chinese Centre of Disease Control and Prevention published a study conducted on 44672 confirmed cases of COVID-19. It was concluded that 81 percent of the corona infected people had mild symptoms, 14 percent of the remaining were in severe conditions while five percent experienced critical illnesses like respiratory failure, septic shock or multiple organ failure. Also, only 2.2 percent of confirmed cases were less than 20 years old.
Preliminary researches on corona illustrate that elderly or people with comorbidities like cardiovascular diseases diabetes mellitus, cancer, hypertension, or lung diseases are at higher risk(Thevarajan et al., 2020; Zheng, Ma, Zhang, & Xie, 2020).The very first study conducted on 41 covid19 laboratory confirmed cases showed that 28 patients were discharged and six had died. Jordan et al. described that around 25 percent of people including adults more than 70 years and those having existing health problems like respiratory disorders, cancer and cardiovascular diseases in United Kingdom are designated in high risk category (Jordan, Adab, & Cheng, 2020). Chen et al. conducted a study on a cohort of 799 corona-affected patients admitted in the isolation ward of a hospital in Wuhan, China(Chen et al., 2020).The authors compared characteristics of 113 death cases with those of 161 recovered cases. Study concluded that the patients who died were around 17 years older than the patients who recovered. 83.7 percent of the deceased were males and had comorbidities like hypertension, cardiovascular diseases and diabetes mellitus etc. The review of literature reveals that in most of the patients admitted with medical comorbidities of SARS-CoV-2, a wide range of clinical manifestations can be seen.
In response to the recent novel coronavirus outbreak originating in Wuhan, Hubei province, China, observations concerning novel coronavirus mortality are of urgent public health importance. The present work presents the first review of the fatal novel coronavirus cases in China. Clinical data of fatal cases published by the Chinese Government were studied. As of 2 February 2020, the clinical data of 46 fatal cases were identified. The case fatality rate was significantly higher in Hubei province than the rest of China. While 67 percent of all deceased patients were male, gender was unlikely to be associated with mortality. Diabetes was likely to be associated with mortality.
There is, however, not yet sufficient evidence to support the association between hypertension and mortality as similar prevalence of hypertension was also observed in the Hubei population In response to the recent novel coronavirus outbreak originating in Wuhan, Hubei province, China, observations concerning novel coronavirus mortality are of urgent public health importance. The present work presents the first review of the fatal novel coronavirus cases in China. Clinical data of fatal cases published by the Chinese Government were studied. As of 2 February 2020, the clinical data of 46 fatal cases were identified. The case fatality rate was significantly higher in Hubei province than the rest of China. While 67 percent of all deceased patients were male, gender was unlikely to be associated with mortality. Diabetes was likely to be associated with mortality.
There is, however, not yet sufficient evidence to support the association between hypertension and mortality as similar prevalence of hypertension was also observed in the Hubei population In response to the recent novel coronavirus outbreak originating in Wuhan, Hubei province, China, observations concerning novel coronavirus mortality are of urgent public health importance. The present work presents the first review of the fatal novel coronavirus cases in China. Clinical data of fatal cases published by the Chinese Government were studied. As of 2 February 2020, the clinical data of 46 fatal cases were identified. The case fatality rate was significantly higher in Hubei province than the rest of China. While 67 percent of all deceased patients were male, gender was unlikely to be associated with mortality. Diabetes was likely to be associated with mortality.
There is, however, not yet sufficient evidence to support the association between hypertension and mortality as similar prevalence of hypertension was also observed in the Hubei population In response to the recent novel coronavirus outbreak originating in Wuhan, Hubei province, China, observations concerning novel coronavirus mortality are of urgent public health importance. The present work presents the first review of the fatal novel coronavirus cases in China. Clinical data of fatal cases published by the Chinese Government were studied. As of 2 February 2020, the clinical data of 46 fatal cases were identified. The case fatality rate was significantly higher in Hubei province than the rest of China. While 67 percent of all deceased patients were male, gender was unlikely to be associated with mortality. Diabetes was likely to be associated with mortality.
There is, however, not yet sufficient evidence to support the association between hypertension and mortality as similar prevalence of hypertension was also observed in the Hubei population. A series of viral pneumonia cases were confirmed in Wuhan, Hubei province, China in December 2019. A new coronavirus was identified and named by the World Health Organization first as 2019-nCoV then SARS-CoV-2 as the cause of the disease COVID-19. While the pathogenesis and aetiology of SARS-CoV-2 infection is still not completely known, it has been observed that it is genetically similar to
SARS-CoV and MERS-CoV
And that the incubation time is between 1 and 14 days.
Unlike other human coronaviruses, some patients had low-grade fever or were even asymptomatic yet remained infectious.
Recently, snakes have been suggested as the natural reservoirs of SARS-CoV-2, assuming that the Huanan Seafood Wholesale Market was the origin of the virus
Methodology
The present study was conducted using different sources like the corona-tracker India, which is updated daily based on the data displayed on the website of Union Ministry of Health and Family Welfare; press releases of different states; directorate of health services of various state Governments; official government links; databases PubMed and Web of sciences until April 10, 2020.We collected data pertaining to demographic, epidemiological, clinical and laboratory characteristics of deceased patients along with their medical history, travel and exposure history and underlying chronic diseases if any. The first 206 death cases were thoroughly analysed to delineate the clinical characteristics and evaluate the prevalence of underlying comorbidities if any, in corona victims in India.
Results
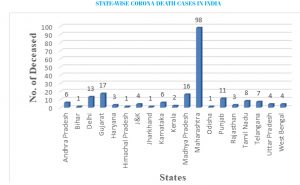
The results of the present study depicted that as on 10th April 2020 (Ministry of Health and Family Welfare site, accessed on 10 April 2020, 08:00 GMT+5:30) the number of deceased cases was the highest in Maharashtra (98) followed by Gujarat (17), Madhya Pradesh (16), Delhi (13) and Punjab (11). State-wise deceased cases in India is depicted in figure 1. It was found that 5.1 percent of the deceased were less than 40 years old while 53.4 percent were more than 60 years old and 41.4 percent were between 40 to 60 years old. Age-wise deceased cases are shown in figure 2. 72.3 percent (149) of the deceased were males whereas 27.7 percent were females i.e. death ratio of males to females was 2.6:1. This shows that male sex is more prone to corona virus infection than females.
This is presented in 10.6 percent (22) of the deceased were diabetic and 7.7 percent (16) were hypertensive. 22.3 percent (46) of the dead patients were diabetic as well as hypertensive. 8.7 percent (18) of the deceased were having pre-existing respiratory problems. All three conditions i.e. diabetes mellitus, hypertension and cardiovascular disease were present in 4.8 percent (10) of the deceased patients. Percentage of co-morbidities in CORONA deceased cases is depicted in figure 4 below. 9.7 percent (20) of the deceased patients were having travel history from the affected regions. 3.8 percent (8) deceased were associated with Tablighi Jamaat who attended religious ceremony in Delhi. The youngest causality of corona in India was fourteen months old boy from Gujarat’s Jamnagar who died of multiple organ failure. A thirty-year-old pregnant woman is the first and only case to die of corona virus infection during pregnancy in India. She was nine months pregnant and had pre-existing respiratory complications.
Fever and cough were the predominant symptoms at the onset. Some other prevalent clinical manifestations in deceased patients included fatigue, chest tightness, head ache, sore throat and dyspnoea while few less common symptoms were diarrhoea, myalgia and anorexia. Acute respiratory distress syndrome, respiratory failure, cardiac failure, sepsis and renal failure were some of the common complications that were observed in the deceased.
Discussion and conclusion. Around 53.4 percent of deaths included a person aged above 60 years which shows that older people are at significantly higher risk of developing corona infection. Reasons that older people are more susceptible to corona include various physiological changes that occur in the body with ageing. In addition to this, body’s immune function decreases with age and multi-morbidity thus making older people more vulnerable to the infection and other serious complications. They are also more prone to have conditions like cardiac and lung disease, diabetes mellitus or renal problems that weaken the ability of their body to fight with infectious disease. But there are some reports showing that people above 60 years who were admitted to hospitals for corona treatment have recovered completely.
Therefore, it is evident that the health of a person before the pandemic plays a crucial role. People who are healthy and free from any medical conditions are at lesser risk. Another pattern that is being observed in this research is gender differences i.e. males seem to hit harder and are more likely to have severe illness than females. This may be because of biological differences between men and women. Immune responses in women are more robust as compared to men. Also since autoimmune diseases are more prevalent in women, they are more protected against new invading infections because of production of increased levels of antibodies that remain in the circulation for a longer time. Toll-like receptor (TLR)-7 is also higher in females leading to better immune responses and ultimately increased resistance to viral infections (Conti & Younes, 2020). Another factor is that the presence of two X chromosomes in women emphasizes their immune system though only one is inactive, while there is only one X chromosome in men (Conti & Younes, 2020; Sawalha, Zhao, Coit, & Lu, 2020). A research on single-cell sequencing concluded that that ACE2 (Angiotensin Converting Enzyme 2) gene expression was more predominant in males in Asia, which may be the reason that men are more susceptible to corona (Corley & Ndhlovu, 2020).
Severe acute respiratory syndrome coronavirus (SARS-CoV) and SARS-CoV-2 bind to their target cells through Angiotensin converting enzyme 2 receptors (ACE2), which is expressed by epithelial cells of the lungs, kidneys, intestine and blood vessels which significantly increases in patients having type 1 or type 2 diabetes mellitus, treated with “ACE inhibitors (ACEIs) and angiotensin II type-I receptor blockers (ARBs)” (Wan, Shang, Graham, Baric, & Li, 2020). The ACE inhibitors and ARBs used for the treatment of hypertension may results in an upregulation of Angiotensin converting enzyme 2 ACE2(X. C. Li, Zhang, & Zhuo, 2017). Thiazolidinediones and ibuprofen can also increase ACE2. This shows that ACE2 expression is increased in diabetes mellitus and treatment with ACE inhibitors and ARBs increases ACE2 expression facilitating corona infection (Fang, Karakiulakis, & Roth, 2020).
It is also observed in our study that patients with cardiovascular diseases are more vulnerable for novel coronavirus infection. Previous studies also depicted relationship between cardiovascular metabolic diseases and SARS and MERS infections (Badawi & Ryoo, 2016; Yang et al., 2006). The reports of ACE2 gene expression in cardiovascular system poses a greater risk to the patients with existing cardiovascular diseases if contracted with corona infection and also affect the development and prognosis of pneumonia. Therefore, we suggest that patients with cardiovascular diseases, diabetes mellitus and hypertension who are treated with ACE2 related drugs, are at higher risk for developing corona infection. They should be carefully monitored for ACE2-modulating medications. Our research concludes that pre-existing comorbidities like diabetes, hypertension, respiratory and cardiac problems are strongly associated with poor outcome in corona-affected patients. Patients having cardiovascular comorbidities are more susceptible to develop cardiac complications which highlights the significance of earlier cardiac monitoring and supportive care in such patients. To conclude we believe that strict monitoring and classification of corona patients with comorbidities could help in the individual evaluation of the disease and would provide effective triage for the treatment and management of individual patients.
Some aspects of RAS and CORONA
The connecting link to this associated comorbidity has been the angiotensin-converting enzyme-2 (ACE2) receptor as its site of virus multiplication. Research has proved that ACE2 is expressed in epithelial cells of the lung, intestine, kidney and blood vessels. The expression of ACE2 is substantially increased in patients with diabetes, hypertension and it is the regulator not only of the blood pressure, but inflammation and immune mechanisms too.
One of the strategies emerged was to consider the use of ACE 1 inhibitors and ARBs drugs during the treatment and management of corona infection. Another strategy has been to develop antiviral newer drugs including the repurposing of the available drugs considering the ACE2 as the target. In spite of all these attempts, the death rates are not getting decreased. Further, some of the clinical features appear to be similar throughout the world.
ACE2 is found in epithelial cells of the lung, intestine, kidney and blood. Increase in ACE2 has been reported in patients with type 1 or type 2 diabetes and hypertension and may be responsible for cardiomyopathy. In patients having type 1 or type 2 diabetes mellitus, if treated with ACE inhibitors and angiotensin II type-I receptor blockers (ARBs) have increased levels of ACE2.
It is also observed in our study that patients with cardiovascular diseases are more vulnerable for novel coronavirus infection. Patients with existing cardiovascular diseases face a greater risk of corona infection and also affect the development and prognosis of pneumonia. Pneumonia leads to substantial gas exchange obstruction, causing hypoxaemia, which diminishes the energy supplied by cell metabolism and upsurges anaerobic fermentation. This causes destruction of phospholipid layer of cell membrane by intracellular acidosis and oxygen free radicals causing respiratory distress and it is the primary cause of corona-induced death.
ACE 1 or the Angiotensin per se may not have a direct role with COVID-19 multiplication, but its binding to ACE2 or the site is likely to cause disturbance in the regulation and function of RAS. Besides blood pressure control by angiotensin-1 orangiotensin-2, both are involved in immune mechanisms cytokines control. Even the porphyrin and methhemoglobin like situation is likely to be produced with the disturbances in RAS.
It may be assumed that as a consequence to this, there may be exaggerated increased in the expression of ACE2 that facilitates infection with COVID-19. It is suggested that patients with cardiovascular diseases, diabetes mellitus and hypertension who are treated with ACE2 related drugs have the worst prognosis after corona infection. They should be monitored carefully for ACE2-modulating medications. During the management of the patients in ICU, RAS should be considered not only from the point of new drug usage for the treatment of the patient but also the management of the serious patient of corona in ICU.
It is necessary to consider holistically the role of RAS when the ACE2 receptors are occupied by corona. There is a controversy whether the ACE2 levels are increased or inhibited. There are no therapeutically proven inhibitors of ACE2. Angiotensin receptor blockers like losartan block vasoconstrictor and profibrotic through AT1 receptors, but in turn they cause activation of AT2 receptors to produce vasodilatation. It is not clear whether because of corona there is inhibition of just receptors of ACE2 or ACE2 levels. It is well known that physiologically, there is short feedback control through renin on ACE2 production. Further, ACE2 is also reported to be generated through an alternate pathway in heart and kidney. The same possibility cannot be ruled out in abnormal circumstances in lung tissues. ACE2 is now known to regulate not only the vasculature but inflammation, oxidative stress, fibrosis and proliferation.
Cytokine surge leading to damage of alveoli and their functions of oxygen transport is one of the main causes of complications leading to multi-organ failure. Further, thrombotic events also appear to be high. These are known to occur in diabetics also and can be correlated with RAS. ACE 2 is known to break down angiotensin-II and angiotensin-I to angiotensin (1–7) and angiotensin (1–9), respectively. ACE2/Ang (1–7) system plays an important anti-inflammatory and anti-oxidant role protecting the lung against infections.
(The authors are from Delhi Pharmaceutical Science and Research University, Delhi)